
Key Takeaways
The 95% failure rate exists because organizations treat AI as a technology problem, when it is actually an organizational and operational problem.
The 5% that succeed follow a clear pattern:
Clinician-centric design → Infrastructure first → Rigorous piloting → Governance → Scale
Real costs run roughly 5× higher than initial budgets because infrastructure, governance, training, and operations are consistently underestimated.
- Typical budget: $800K
- Actual deployment cost: ~$4.1M
Successful deployments typically require ~7 months and strong operational discipline. Compressed timelines strongly correlate with failure.
Healthcare AI success should be measured by patient outcomes, not technical efficiency.
If patient care did not improve, the deployment did not work.
Clinician adoption is the critical success factor.
Roughly 85% of failed projects fail because clinicians do not use the system — not because the AI model underperforms.
Who This Article Is For
- CIOs
- CMIOs
- CTOs
- VPs of Clinical Operations
- Digital transformation leaders
Particularly those evaluating, deploying, or attempting to rescue a healthcare AI initiative.
Introduction
A major U.S. hospital network invested $2.1M in an AI diagnostic assistant in 2024.
The model was excellent.
It achieved 93% accuracy on chest X-ray classification, outperforming radiologists on benchmark datasets.
But by month six, the system was reading 0% of real patient images.
This was not a story about bad AI.
It was a story about strategy without operational infrastructure.
The hospital had a strong vision — deploy AI to improve diagnostics — but lacked the systems required to run AI in production:
- No logging system
- No monitoring
- No governance framework
- No clinician adoption strategy
The scenario above represents a composite pattern drawn from healthcare AI deployment analyses between 2023–2025.
The organization is not named, but the pattern is common.
Today, roughly 95% of healthcare AI deployments fail for the same reason.
Organizations treat AI as a technology project when it is actually an operational transformation.
Real-World Examples of the Failure Pattern
Several high-profile cases illustrate the same structural issue.
IBM Watson for Oncology
IBM invested heavily in healthcare AI through acquisitions including Truven Health, Phytel, Explorys, and Merge Healthcare.
The initiative consumed roughly $5B in healthcare-AI acquisitions before the unit was effectively dismantled and divested in 2022.
Epic Sepsis Prediction Model
A widely cited 2021 study in JAMA Internal Medicine evaluated the sepsis model used in the Epic Electronic Health Record System.
The model:
- Generated alerts for ~18% of hospitalized patients
- Missed 67% of actual sepsis cases
Despite sophisticated algorithms, clinical usefulness was limited.
Generative AI Medical Triage Tools
Independent evaluations of generative-AI medical triage tools have shown that some systems under-triage a substantial portion of genuine medical emergencies.
Again, the issue is rarely the model alone.
The issue is clinical integration and operational oversight.
The Pattern Is Predictable
Healthcare AI initiatives fail because organizations underestimate the operational complexity required to deploy AI safely in clinical environments.
The solution is known.
The organizations that succeed follow a repeatable operational framework.
What We See Across Healthcare AI Engagements
Across healthcare AI deployments involving imaging systems, clinical workflow automation, and AI platforms, the pattern is consistent:
The AI model itself is rarely the failure point.
Failures usually occur in the surrounding operational systems:
- Logging
- Monitoring
- Governance
- Clinician workflow integration
- Change management
Organizations that succeed in production do not necessarily have better AI models.
They have better operational discipline.
The Scale of the Problem: Healthcare’s AI Reckoning
Healthcare organizations are investing billions in AI expecting transformational results.
Instead, they are encountering failure rates that would be unacceptable in most industries.
The Numbers
- ~95% of healthcare AI projects show zero measurable ROI
- ~79% fail to deliver intended clinical outcomes
- ~95% of generative AI pilots never reach production
- ~80% of healthcare AI models fail due to data quality issues
- $58B+ invested in healthcare digital transformation in 2024
Figures drawn from RAND, Bain & Company, Stanford AI Index, and HIMSS healthcare AI research (2023–2025). Individual study methodologies vary; the pattern of single-digit-percentage AI success rates in healthcare is consistent across published research.
But here's what's most revealing:
Organizations that fail and organizations that succeed deploy nearly identical technology.
The difference isn't the AI. It's the operational maturity around the AI.
Real Cost Breakdown: What Healthcare Organizations Actually Spend
Most healthcare leaders budget only for the AI model (~$800K) and assume everything else is included. The actual cost structure across QSS-observed deployments looks materially different.
The cost ranges below are drawn from QSS healthcare AI engagement analyses and corroborating industry research from KLAS, HIMSS, and Bain. Actual costs vary by organization size, existing infrastructure, and AI scope.
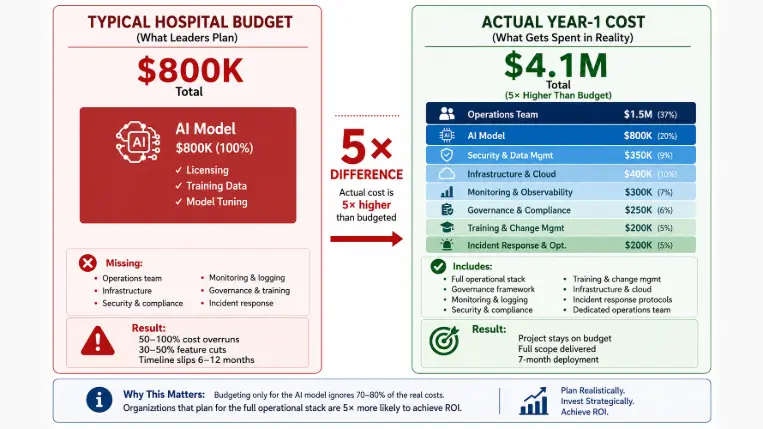
Actual Cost Structure
Component | Year 1 Cost | % of Total |
AI Model (training, licensing, tuning) | $800K | 20% |
Infrastructure & Cloud | $400K | 10% |
Monitoring & Observability | $300K | 7% |
Governance & Compliance | $250K | 6% |
Security & Data Management | $350K | 9% |
Operations Team | $1.5M | 37% |
Training & Change Management | $200K | 5% |
Incident Response & Optimization | $200K | 5% |
Total Year-1 Cost | $4.1M | 100% |
Organizations that budget $800K and expect to deploy cost-effectively are headed for failure. The operational infrastructure costs roughly 5× more than the AI model itself.
Want a tailored Year-1 cost estimate for your healthcare AI deployment? Book a 30-min scoping call with a QSS solution architect →
Why Healthcare AI Deployments Fail: The Four Root Causes
Root Cause 1: Inadequate Clinician Input (Affects ~82% of Projects)
The problem: Organizations build AI in isolation, then expect clinicians to adopt it.
What happens:
- Roughly 82% of clinical AI projects consult clinicians after algorithms are built
- Only about 22% use human-centered design from the start
- Models optimize for benchmark accuracy, not workflow usability
Illustrative example: A hospital implements an AI sepsis alert system. The model achieves 92% sensitivity on test sets. In the ICU, alerts fire for patients already on antibiotics, for fever from non-infectious causes, and for patients already under monitoring protocols. Clinicians disable notifications. The system is never used again.
Root Cause 2: Immature Tools (~77% of Organizations Cite This)
The problem: AI tools work in research settings but fail in real clinical environments.
What happens:
- Bias in training data
- Poor integration with EHR systems
- Vendor tools assume technical expertise clinicians don't have
Illustrative example: An AI trained on 100K academic chest X-rays achieves 92% accuracy on its training dataset. Deployed at a safety-net hospital with different patient demographics, accuracy drops to 67%. The model requires six months of retraining and approximately $400K in additional cost before it's usable in the deployment environment.
Root Cause 3: Infrastructure Failures (~95% Scaling Failure)
Organizations lack:
- Logging and audit trails
- Monitoring systems
- Incident response plans
- Data governance
- Change management
Missing capabilities:
- Every AI decision must be logged for liability
- Performance must be monitored continuously
- Incident protocols must exist for dangerous recommendations
Real cost impact: Organizations spend $800K on the model and then discover they need $1.2M+ in infrastructure. Projects typically experience 30–50% cost overruns at this stage.
Root Cause 4: Governance Vacuum
Healthcare organizations often lack AI governance frameworks. Without governance:
- No approval workflows
- No SLAs for model performance
- No liability clarity
- No regulatory compliance structure
- No clinician oversight
Without governance, deployment freezes — and the AI sits in test environments while teams debate what production should look like.
The 5% That Succeed: What They Do Differently
Organizations that succeed don't necessarily have better AI. They have better operations.

Step 1: Clinician-Centric Design (Weeks 1–4)
Successful organizations:
- Observe real workflows (40+ hours of shadowing)
- Identify clinician pain points
- Design AI around human workflows
- Test assumptions with clinicians before any model training begins
Result: AI integrates naturally into clinical work.
Step 2: Infrastructure First (Weeks 5–12)
Build infrastructure before deploying AI.
Required systems:
- Logging infrastructure
- Monitoring dashboards
- Governance workflows
- Incident response protocols
- Security and compliance controls
You cannot retrofit governance. Organizations that skip this phase fail at scale.
Step 3: Rigorous Piloting (Weeks 13–20)
Successful pilots include:
- Real patient data (not synthetic or benchmark datasets)
- Local clinical workflows
- Early failure-mode detection
- Continuous clinician feedback loops
- Planned model retraining cycles
Step 4: Governance & Training (Weeks 21–28)
Organizations implement:
- Decision protocols
- SLAs for model performance
- Clinician training programs
- Oversight committees
- Feedback loops to model owners
Step 5: Continuous Optimization & Scale (Weeks 29+)
Successful organizations:
- Monitor continuously
- Retrain models quarterly
- Adapt to patient-population changes
- Document validation processes
- Expand gradually — never big-bang
Total timeline: approximately 7 months to production-grade deployment.
Evaluate Your Current Approach: 5 Critical Questions
1. Have you involved clinicians in design?
- Observed workflows and interviewed clinicians
- Consulted clinicians during development
- Building AI first, planning clinician engagement later
2. Do you have infrastructure for logging and governance?
- Logging + monitoring + governance ready
- Partial monitoring
- No infrastructure plan
3. What is your Year-1 budget?
- $4–5M realistic
- $1.5–2M — risk of overruns
- $800K — severely underestimated
4. Are you measuring adoption and outcomes?
- Tracking clinician adoption and patient outcomes
- Planning to track
- Only technical metrics
5. Do you have AI governance?
- Approval workflows and SLAs in place
- Governance in development
- No governance framework
How QSS Approaches Healthcare AI Deployment
QSS focuses on operational discipline, not just AI model selection.
What we've learned across healthcare AI engagements:
- Most failures happen at implementation, not development
- Clinician adoption determines success — even excellent models fail if clinicians work around them
- Infrastructure must exist before the model is deployed, not retrofitted after
- Outcomes must be measured continuously, not at project close
What we aim for in our deployments:
- Production deployment within the planned timeline
- Clinician adoption tracked from day one
- Cost overruns kept under 10% through disciplined scoping
- Year-1 ROI through measured patient outcome improvements
These targets aren't aspirational — they're the difference between the 5% that succeed and the 95% that fail.
Frequently Asked Questions
1.How much does successful healthcare AI deployment cost?
A.$4–5M in Year 1 for a properly architected deployment including AI model, infrastructure, governance, operations team, training, and incident response. Budgets under $1M almost universally produce projects in the 95% failure cohort.
2.How long does deployment take?
A.About 7 months with proper operational discipline — 4 weeks of clinician-centric design, 8 weeks of infrastructure build, 8 weeks of piloting, 8 weeks of governance and training, then continuous optimization. Compressed timelines (under 4 months) correlate strongly with failure.
3.What's the biggest risk factor?
A.Clinician adoption failure. Roughly 85% of failed projects fail because clinicians don't use the system — not because the model underperformed. Adoption planning starts at Week 1, not after deployment.
4.Can we skip infrastructure to move faster?
A.No. Approximately 95% of projects that skip infrastructure-first design fail at scaling. Logging, monitoring, governance, and incident response are not optional — they're regulatory and operational requirements.
5.How do we measure real success?
A.Measure patient outcomes, not just efficiency or model accuracy. Track diagnostic accuracy in production, time-to-treatment improvements, clinician adoption rates, and override rates. If patient care didn't improve, the deployment didn't work — regardless of what the technical metrics show.
6.How often should models be retrained?
A.Typically quarterly for clinical models, more frequently for models with drift-sensitive use cases. Production model performance degrades over time as patient populations and clinical practices evolve.
7.Can AI be deployed without customization to our local environment?
A.No. Expect 4–8 weeks of retraining on local data before any model performs reliably in your specific clinical environment. Models trained on academic medical center data routinely lose 15–25% accuracy when deployed in community or safety-net settings.
8.What happens if AI makes a dangerous recommendation?
A.Organizations must have incident response protocols and governance frameworks in place before deployment. This includes clear escalation paths, mandatory human-in-the-loop on critical decisions, audit logging for every AI inference, and post-incident review processes.
The Bottom Line
Healthcare organizations that succeed allocate budgets like this:
- 20% on the AI model
- 80% on infrastructure, operations, and governance
Organizations that fail allocate the inverse:
- 80% on the AI model
- 20% on everything else
The 5% that succeed treat AI as a workflow problem.
The 95% that fail treat AI as a technology problem.
The framework above is proven. The question is whether your organization has the operational discipline to follow it.
Ready to build healthcare AI that works? Schedule a consultation with a QSS healthcare AI architect → Let's discuss how your organization can be in the 5% that succeed.

About QSS
QSS Technosoft builds production healthcare systems at scale — including AI-driven clinical platforms, DICOM/PACS imaging infrastructure, and HIPAA-aligned cloud deployments. Our healthcare practice focuses on the operational disciplines that determine whether AI deployments succeed or fail in production environments.
Learn more: QSS Healthcare Solutions →
Why 95% of Healthcare AI Deployments Fail (And the 5-Step Framework That Works)