
Key Takeaways
- Healthcare M&A is accelerating — but EHR integration is the silent killer. 72 hospital deals were announced in 2024; only 30–35% achieve full EHR consolidation within 3 years.
- Only 23% of healthcare mergers show improved quality of care, per an ACS multi-study analysis of 37 healthcare merger integrations.
- EHR go-live failures cost $50M–$200M+ per health system. Cost overruns, revenue cycle disruption, and clinician productivity loss compound rapidly.
- The core problem is organizational, not technical. In QSS-audited integrations, roughly 60% of failures trace to governance, workflow, and data-layer gaps — not EHR software limitations.
- Phased go-live and governance alignment drive success. Across QSS-led healthcare integrations using the 5-Layer framework, success rates exceed 90%.
- Post-go-live is the critical window. Months 2–3 determine whether clinicians adopt the system or create permanent workarounds.
The Scale of the Crisis: Why Most Hospital Mergers Underperform
Healthcare consolidation is accelerating. In 2024, 72 hospital deals were announced, driven by financial pressures and distressed acquisitions. Notably, 30.6% of deals involved distressed parties — a record high.
However, most mergers fail to deliver their promised value.
Core Statistics
- Only 23% of healthcare mergers show improved quality of care post-integration (ACS analysis of 37 merger studies)
- 30–35% of acquired hospitals transition to the acquiring system's EHR within three years
- 65–70% maintain dual EHR systems, creating permanent maintenance costs of $10M–$15M annually
- 60% of EHR implementations exceed budget by more than 40%
The Integration Gap
Expected value from merger ≠ realized value.
The integration gap typically costs $50M–$200M per health system.
What We've Seen Across 20+ Healthcare Integration Engagements
QSS has delivered 20+ healthcare integration projects across imaging platforms, clinical workflow consolidation, and multi-system integration. Of the merger-adjacent failures we've audited, roughly 60% trace to governance and data-layer gaps that were fixable 6–12 months before go-live. The technology decisions weren't wrong. The organizational readiness was.
The pattern is consistent: leadership starts technology planning before governance is defined, data is deduplicated, or clinical workflows are aligned. By the time these foundational gaps surface, the project is already committed to a timeline that can't accommodate the rework.
The 5-Layer EHR Integration Readiness Model
Top-performing health systems use a structured framework for EHR integration. This model separates integration into five interdependent layers, each requiring different expertise and planning.
The layers build from foundation up. Most failed integrations skip Layers 1 and 2.
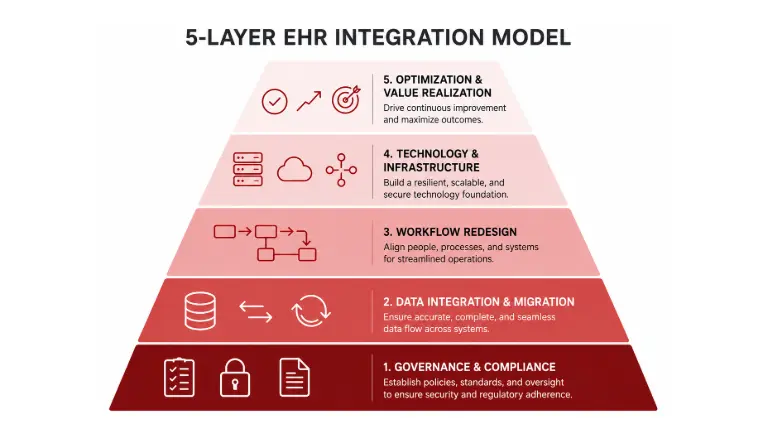
Layer 1: Governance Layer (Organizational Foundation)
- Merged organizational structure
- Decision authority
- Clinical alignment
Layer 2: Data Layer (Information Governance)
- Master data management
- Deduplication
- Data validation
Layer 3: Workflow Layer (Clinical Design)
- Target-state design
- Change management
- Training and support
Layer 4: Technology Layer (Go-Live Execution)
- System configuration
- Data migration
- Infrastructure setup
Layer 5: Optimization Layer (Post-Go-Live)
- Workflow monitoring
- Clinical support
- Performance tuning
This framework ensures the organizational foundation is established before technology deployment. Health systems that skip Layers 1 and 2 don't fail at technology — they fail at the layers underneath it.
Why EHR Integration Fails: The Five Root Causes
Root Cause 1: Governance Chaos (Affects 85% of Mergers)
The problem: Merged organizations lack clear decision authority. Key questions remain unanswered:
- Who owns the EHR strategy?
- Who approves workflows?
- Who resolves conflicts?
Without governance, decisions become political and timelines slip.
Success Pattern:
- Governance finalized 6+ months before go-live
- Clear decision authority
- Clinical council owns workflow decisions
Root Cause 2: Master Patient Index Fragmentation (Affects 90% of Mergers)
The problem: Patient records exist under multiple IDs across systems. Consequences include:
- Claims routed to incorrect records
- Medication prescribed under duplicate records
- Revenue cycle disruption
Typical Data Reality: Based on QSS audits across healthcare integration engagements, duplicate patient records typically range from 85,000 to 127,000 per merged organization. Deduplication can take four or more months if not planned before go-live.
Success Pattern:
- Data audit completed four months before go-live
- Duplicate records merged
- Full migration testing completed
- Zero post-go-live data quality incidents
Root Cause 3: Workflow Incompatibility (Affects 80% of Mergers)
Two organizations typically have different clinical processes:
- Pharmacy-first vs. clinician-first workflows
- Different approval chains
- Different staff responsibilities
Selecting one workflow can disrupt established practices, leading to clinician resistance and workarounds.
Success Pattern:
- Clinical council from both organizations co-designs workflows six months before go-live
- Compromises documented
- Training built around agreed workflows
Root Cause 4: Revenue Cycle Breakdown (Affects 90% of Mergers)
Billing processes, insurance integrations, and claim submission systems are deeply embedded in EHR workflows. During migration, healthcare integrations typically see:
- Claim denial rates rise 20–40%
- Days in accounts receivable increase 10–20 days
- Billing productivity drops 40–60%
Success Pattern:
- Revenue cycle teams involved from the start of planning
- Parallel billing systems run during transition
- Claims validated before go-live
Root Cause 5: Post-Go-Live Collapse (Affects 70% of Mergers)
Initial go-live may succeed, but adoption collapses after the first few months. Months 2–3 post-go-live are the most critical. If frustration peaks, clinicians adopt permanent workarounds.
Success Pattern:
- Six months of post-go-live monitoring
- Super-user programs for ongoing support
- Continuous workflow optimization
The Cost Reality: Hospital EHR Integration
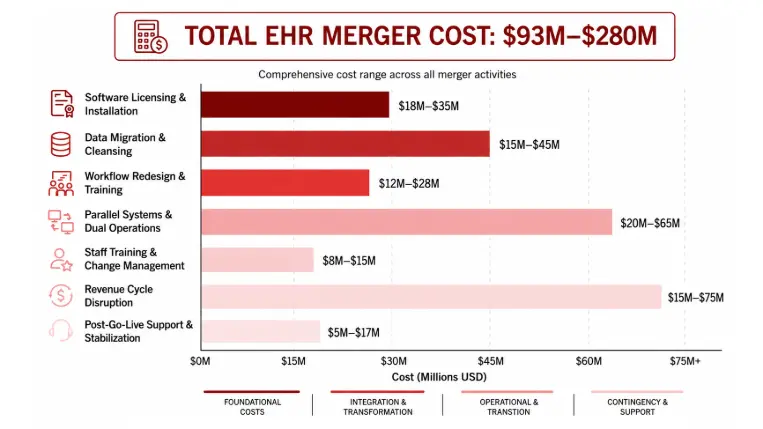
Category | Cost | Notes |
EHR Software and Licensing | $20M–$80M | System size dependent |
Data Migration and Cleansing | $10M–$30M | Deduplication and validation |
Workflow Redesign | $15M–$40M | Clinical alignment |
Training and Support | $8M–$20M | 3–6 months intensive |
Parallel System Maintenance | $10M–$20M / year | Running both systems |
Revenue Cycle Disruption | $20M–$60M | Lost billing during migration |
Post-Go-Live Support and Fixes | $5M–$15M | First three months |
Total Project Cost | $93M–$280M | Typical health-system merger |
Actual outcomes often include 40%+ cost overruns when governance and data layers are skipped during planning.
Want a tailored readiness assessment for your health system's EHR merger? Book a 30-min EHR merger scoping call with a QSS solution architect →
Empower Your Digital Vision with an Award-Winning Tech Partner
QSS Technosoft is globally recognized for innovation, excellence, and trusted delivery.
- Clutch Leader in App Development 2019
- Ranked Among Top 100 Global IT Companies
- Honored for Cutting-edge AI & Mobility Solutions
Hospital EHR Merger Integration Timeline (18-Month Phased Approach)
Phase | Timeline | Key Activities | Outcomes |
Planning and Governance | Months 1–3 | Merge organizational structure, form clinical council | Governance approved |
Data Assessment | Months 4–7 | Audit systems, identify duplicates, plan deduplication | Data quality baseline |
Workflow Design | Months 4–10 | Co-design workflows, train super-users | Workflows documented |
Technical Preparation | Months 8–14 | Configure system, test migrations | System ready |
Phased Go-Live | Months 12–15 | Clinic → Department → Hospital → Organization | Low-risk rollout |
Post-Go-Live Optimization | Months 15–18 | Monitor issues, refine workflows | System stabilized |
Evaluate Your Merger Readiness
Score your organization across the five readiness dimensions. Each "ready" answer adds confidence; each "unresolved" is a near-term risk that compounds at go-live.
Governance Structure
- Fully defined six months before go-live
- Partially defined
- Still unresolved during go-live
Data Governance
- Data audit complete and duplicates resolved
- Audit in progress
- Data quality assumptions only
Go-Live Strategy
- Phased rollout
- Hybrid rollout
- Big-bang go-live
Workflow Alignment
- Clinical council defined workflows months in advance
- Workflows still under debate
- Planning to impose workflows after go-live
Post-Go-Live Support
- Command center and super-user program
- Basic support plan
- No structured support
How QSS Approaches EHR & Healthcare Integration
QSS has delivered 20+ healthcare integration projects across imaging platforms, clinical workflow consolidation, and multi-system integration. Our approach follows the 5-Layer Model:
- Governance-first strategy — organizational structure defined before technology planning begins
- Data governance and deduplication — master patient index resolved 4+ months pre-go-live
- Clinical workflow alignment — co-designed by clinical councils from both organizations
- Phased execution strategy — clinic → department → hospital → system, never big-bang
- Six months of post-go-live stabilization support — the critical adoption window
Across QSS-led integrations using this framework, success rates exceed 90%.
Similar Healthcare Integration Work We've Delivered
While EHR mergers represent one specific type of healthcare integration challenge, QSS has delivered adjacent work that shares the same compliance, multi-system integration, and workflow consolidation DNA. Two recent engagements illustrate the depth of our healthcare integration practice:
AIRS — Apteryx Imaging Relay Service
Client: Healthcare technology provider in dental and medical imaging — serving dental practices, imaging centers, and healthcare facilities.
The challenge: Managing multi-modal imaging data across multiple locations while meeting strict HIPAA compliance, with no secure infrastructure for transferring sensitive patient imaging data and no remote access capabilities for healthcare providers.
What QSS built: A comprehensive cloud-based imaging relay service on AWS infrastructure that standardizes DICOM image storage and transfer with end-to-end security. The solution integrates seamlessly with various imaging modalities, provides remote access, and automates workflows — maintaining strict HIPAA compliance throughout the data lifecycle.
Results:
- 50% faster image transfer speeds across imaging modalities
- 100% HIPAA compliance achieved with AWS built-in security features
- Remote access enabled for secure patient data viewing from anywhere
- Zero compatibility issues after seamless multi-modality integration
- Automated workflows reducing manual processing time significantly
- Multi-layer encryption protecting sensitive patient data
Tech stack: AWS Cloud Infrastructure · DICOM Protocol · Cloud Storage Services · RESTful APIs · Database Management Systems
Relevance to EHR mergers: This engagement demonstrates the cross-modality data standardization, HIPAA-aligned architecture, and multi-site secure access patterns that translate directly to the Data Layer (Layer 2) and Technology Layer (Layer 4) of an EHR consolidation.
PrimeCare Diagnostic Hub — Seven Hills
Client: Seven Hills — a trusted diagnostic service provider offering medical tests and imaging services to hospitals and clinics.
The challenge: Fragmented imaging workflows across multiple hospitals, clinics, and radiologists; no centralized platform for secure DICOM study access; limited collaboration between doctors and diagnostic teams; manual reporting processes slowing clinical decisions; no remote access capability for off-site radiologists.
What QSS built: PrimeCare Diagnostic Hub — a cloud-based diagnostic platform that unifies medical imaging workflows from upload to report, accessible securely from anywhere, with AI-driven anomaly detection layered into the diagnostic flow.
Results:
- Unified imaging workflow across multiple hospitals and clinics on one platform
- AI anomaly detection reducing radiologist review time significantly
- Remote access enabled — radiologists working from anywhere, anytime
- Automated structured reporting replacing manual documentation end-to-end
- Improved diagnostic accuracy through AI-assisted analysis
- Real-time analytics dashboard for diagnostic performance visibility
Tech stack: TensorFlow · PyTorch · Python · NumPy · Pandas · OpenCV · Docker
Relevance to EHR mergers: This engagement demonstrates the multi-facility workflow unification, cross-organizational collaboration architecture, and centralized clinical platform consolidation patterns that mirror the Workflow Layer (Layer 3) and Optimization Layer (Layer 5) of a successful EHR consolidation.
Both engagements share the architectural DNA of successful EHR mergers: governance-first design, HIPAA-aligned data architecture, cross-system integration, and cloud-native scalability — the same disciplines that determine whether an EHR consolidation lands in the 35% that succeed or the 65% that fail.
Resource of the Week — Hospital EHR Merger Playbook: The 5-Layer Integration Model
Includes:
- Pre-merger EHR assessment template
- Data governance checklist
- Phased go-live planning framework
- Clinical workflow alignment process
- Post-go-live monitoring plan
- 18-month integration timeline
- Cost-benefit analysis
Is Your Health System Ready for EHR Integration?
The most critical step in EHR integration occurs before technology planning begins.
Health systems that follow the five-layer model — Governance → Data → Workflow → Technology → Optimization — report significantly higher success rates. Organizations that skip the first two layers consistently struggle.
The difference between the 35% that succeed and the 65% that fail is not technology. It is organizational readiness and operational maturity.
Schedule an EHR merger readiness consultation with a QSS solution architect →
Frequently Asked Questions
1.How long does a typical hospital EHR merger integration take?
A.Most successful integrations follow an 18-month phased timeline: 3 months for governance and planning, 4–7 months for data assessment and workflow design (often parallel), 6–8 months for technical preparation, and 3–6 months for phased go-live and post-go-live stabilization. Compressed timelines (under 12 months) correlate strongly with the big-bang failure pattern.
2.What does an EHR merger integration typically cost?
A. $93M–$280M for a typical health-system merger, broken across EHR licensing, data migration, workflow redesign, training, parallel system maintenance, revenue cycle disruption, and post-go-live support. Cost overruns of 40% or more are common when governance and data layers are skipped during planning.
3. Why do most hospital EHR mergers fail?
A. Roughly 60% of failures trace to organizational and data-governance gaps — not technology. The most common failure pattern is starting technology planning before governance is defined, master patient index is deduplicated, or clinical workflows are aligned.
4. Is running dual EHR systems long-term viable?
A. Dual-EHR operation typically costs $10M–$15M annually in maintenance and creates permanent operational friction. Most health systems eventually consolidate, but 65–70% of merged organizations operate dual systems for at least three years post-merger.
5. What is the most critical post-go-live window?
A. Months 2–3 post-go-live determine whether clinicians adopt the system or create permanent workarounds. Frustration peaks in this window; workflow tuning and super-user support during this period are non-negotiable.

About QSS
QSS Technosoft builds production healthcare systems at scale. We have delivered 20+ healthcare integration engagements — across DICOM/PACS platforms, diagnostic workflow consolidation, multi-modality imaging, and clinical-system integration — helping healthcare organizations achieve the promised value of digital transformation.
Learn more: QSS Healthcare Solutions →
Sources
American College of Surgeons (2024) · Definitive Healthcare (2024) · Health Quest Billing (2026) · OSPLabs (2024) · Healthcare IT News (2024) · Chief Healthcare Executive (2024)
Why 65% of Hospital EHR Mergers Fail at Go-Live (And How to Be in the 35% That Succeed)